Medical hypnosis: a multifaceted tool

Although there is currently no consensus on the descriptions of hypnosis, many researchers and theorists agree with the American Psychological Association’s (APA) definition, which defines hypnosis as “a state of attention involving focused attention and a reduction in peripheral awareness, characterized by an increased susceptibility to suggestion ” [1]. This definition comprises three main components:
- Absorption: The ability to become fully immersed in a mental or imaginary image. Example: The practitioner guides you through visualizing an imaginary landscape. You see vivid details, feel the cool air on your skin, and hear birds singing. You are so absorbed in this imaginary scene that you momentarily forget your real surroundings.
- Dissociation: A functional separation between psychological or mental elements that are usually connected. Example: The practitioner helps you focus your attention on a sensation lightness in one part of your body. Meanwhile, you feel as if the pain another part of your body is disconnected from you. This dissociation allows you to manage the pain by reducing your perception of it.
- Suggestibility: An increased tendency to follow the practitioner’s instructions. Example: The practitioner suggests that you feel a sensation warmth and comfort in the painful area of your body. You follow this suggestion and actually feel this soothing warmth, which helps reduce the pain.
Over the years, hypnosis has evolved into a valuable therapeutic tool. Today, medical hypnosis helps treat a wide range of conditions—from stressanxiety to chronic pain—by guiding the patient toward their own resources and solutions.
This article specifically explores medical hypnosis from various perspectives. After providing a precise definition of this practice, we will delve into the brain mechanisms underlying its therapeutic effects. Finally, we will review the main clinical applications of medical hypnosis.
Medical Hypnosis vs. Hypnotherapy
Before getting to the heart of the matter, it is important to understand the difference between the terms “medical hypnosis” and “hypnotherapy.” Although these terms are sometimes used interchangeably, they refer to two distinct practices.
Hypnotherapy is generally practiced in private practices by trained and certified doctors or psychologists and is aimed at personal development, well-being, or psychological support (such as smoking cessation). It encompasses various approaches and techniques (analytical, dream-based, cognitive-behavioral, etc.), which do not always have formal scientific validation.
Medical hypnosis, on the other hand, is practiced in hospitals, private clinics, or doctors’ offices and is intended to treat specific medical conditions. It is performed by healthcare professionals (psychologist, nurse, doctor ) who have completed additional training in medical hypnosis in addition to their Training . It is subject to the strict regulations of the medical profession and is based on validated and standardized medical protocols as well as scientific research. Medical hypnosis may be partially or fully covered by health insurance, depending on the health issue being treated and individual insurance policies.
Medical hypnosis draws on both formal hypnosis (a traditional practice based on direct suggestions) and conversational hypnosis (in which the hypnotic state is induced indirectly during what appears to be a “conversation”) [2]. Figure 1 below illustrates the sequence of events during a session:
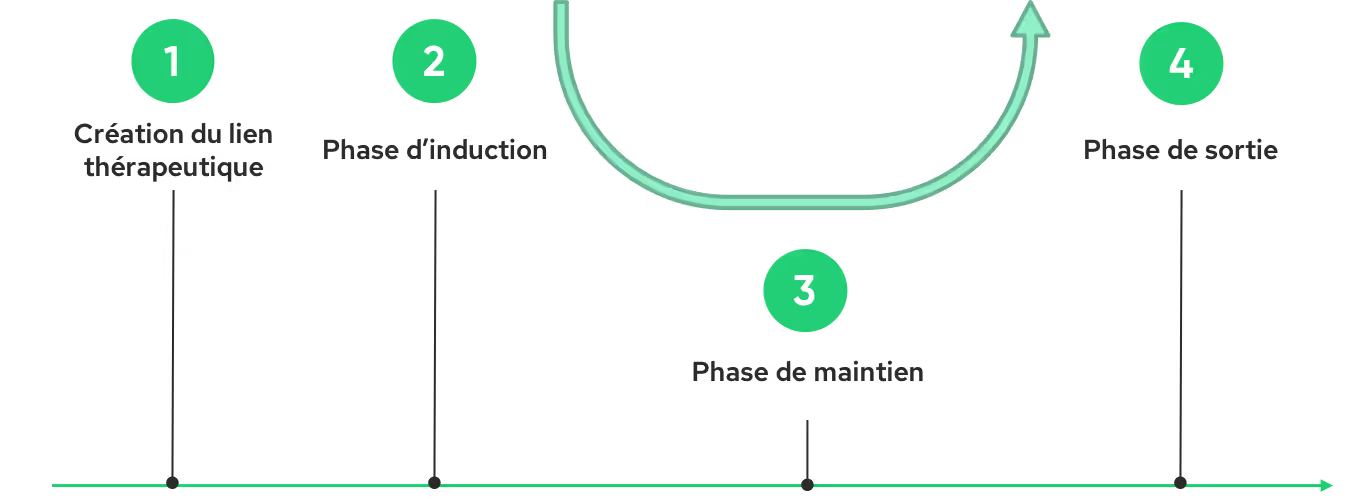
Establishing the therapeutic bond between the practitioner and the patient is the first essential step toward a successful hypnosis session. This relationship, based on empathy and clear communication, creates an atmosphere conducive to relaxation openness to suggestions. The induction phase that follows aims to guide the patient into a hypnotic state conducive to receiving suggestions. The practitioner then uses various techniques: verbal suggestions, guided visualizations, and breathing exercises. Once this state is achieved, the maintenance phase allows the hypnotic state to be deepened and specific therapeutic suggestions to be introduced. For example, when managing pain, the practitioner may invite the patient to visualize their pain an entity detaching from their body and then gradually fading away. These suggestions, reinforced by metaphors and analogies, aim to alter the perception of pain promote a state of well-being. Finally, the emergence phase allows the patient to be gradually brought back to a normal state of consciousness, while encouraging them to internalize the benefits of the session. The practitioner may suggest that the patient hold onto the feelings of calm and well-being experienced during the session and draw upon them when needed.
What happens in the brain?
Thanks to advances in neuroimaging, we are beginning to identify the brain regions associated with the hypnotic state. Medical hypnosis makes it possible to modulate brain activity in regions involved in self-awareness, mental imagery, emotion regulation, attention, and pain perception pain for a more in-depth review, see [3]).
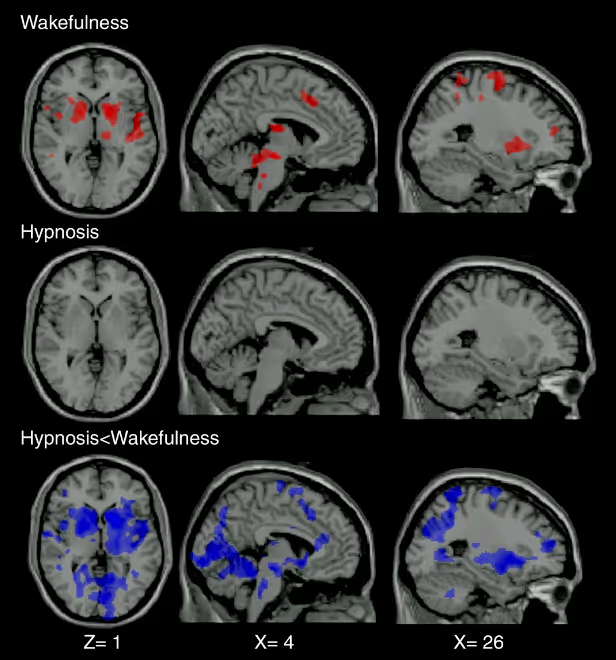
The authors of a 2009 study investigated differences in brain activation induced by painful and non-painful stimuli in healthy subjects under hypnosis and in a normal waking state [4]. While painful stimuli during wakefulness predictably activated regions involved in pain perception, these same stimuli, when administered under hypnosis, did not result in significant activation of these regions (Figure 2). The bottom row of Figure 2 compares the activation patterns between the normal waking state and the hypnotic state. The regions activated during painful stimulation (shown in blue in the figure) are significantly less active under hypnosis than in the normal waking state. These results suggest that hypnosis may significantly modulate the brain processes involved in pain perception.
Beyond the activity of these regions, hypnosis also alters the way these different regions communicate with one another [5]. Some connections are strengthened, while others are weakened. These changes in functional connectivity may explain the various effects of hypnosis, such as pain reduction, improved concentration, or altered sensory perceptions. Furthermore, hypnosis may also promote the release of neurotransmitters such as dopamine, serotonin, and endorphins, which play a role in regulating mood, pain relaxation 6].
It is important to note that these findings are based on ongoing research and that our understanding of hypnosis is constantly evolving.
Medical Applications
Hypnosis can be used in many clinical settings to help manageanxiety, pain sleep disorders. It thus contributes to significantly improving the well-being and quality of life of patients of all ages, from children to the elderly. The methods used are tailored to each age group. Published in 2015 by the Sparadra association, the“Practical Manual of Hypnoanalgesia for Pediatrics Care” by Bénédicte Lombart and her colleagues offers a range of practical tools for implementing hypnoanalgesia ( pain management) in children. In particular, this guide provides scripts tailored to each age group, using simple language and familiar metaphors to support young patients. More recently, in 2024, Geneviève Perennou and Serge Sirvain coordinated the development of a checklist specifically designed for elderly people. This tool lists the hypnotic techniques best suited for this population, thus offering professionals a valuable resource for supporting these individuals.
Currently, the use of medical hypnosis for pain management is the application with the highest level of scientific evidence. In fact, hypnosis can reduce the perception of pain (burn care, injections, Dental care, etc.) [7], chronic pain [8], and post-surgical pain [9] in many clinical settings. It can also help pregnant women manage pain anxiety pregnancy and childbirth [10].
In addition to anesthesia or sedation (hypnosedation), medical hypnosis can reduceanxiety, pain medication use in the operating room, while speeding up postoperative recovery [11]. The effectiveness of hypnosis varies depending on individual suggestibility [12]. A study involving 3,632 patients showed that hypnosis reduced pain 42% in highly suggestible subjects and by 29% in moderately suggestible subjects [13]. Even the least suggestible patients benefit, albeit to a more limited extent.
The use of hypnosedation in conjunction with general or local anesthesia is recommended by the SFAR (French Society of Anesthesia and Intensive Care).

🎥 If you’d like to learn more about the use of medical hypnosis in hospitals, we recommend watching the Belgian documentary *Ma voix t'accompagnera*, released in 2020 on Netflix. This film explores how two Belgian anesthesiologists, Fabienne Roelants and Christine Watremez, use hypnosis in the operating rooms at the Cliniques Saint-Luc in Brussels.
When it comes to managinganxiety, studies show that hypnosis can significantly reduceanxiety , thereby improving the overall patient experience for both adults and children [9]. Patients undergoing invasive or painful medical procedures, such as endoscopies [14], biopsies [15], and colonoscopies [16], may also benefit from hypnosis to reduce their anxiety. A meta-analysis was conducted in 2019 to evaluate the effectiveness of hypnosis in treatinganxiety 17]. Analysis of the 17 trials included in this study indicates that, on average, individuals who underwent hypnosis therapy achieved better outcomes than 79% of those in the control group. In this study, hypnosis was more effective at reducinganxiety combined with other psychological interventions (cognitive-behavioral therapies, biofeedback, etc.) than when used alone [17].
Hypnosis is particularly indicated for the management of disorders with a psychosomatic component, such as gastrointestinal disorders. In fact, some patients with irritable bowel syndrome may be unresponsive to conventional therapies. A meta-analysis demonstrated that hypnosis is a safe method that provides long-term symptom relief for 54% of patients [18]. Furthermore, it has proven effective in managing symptoms associated with conditions such as cancer (particularly in Palliative care ; [19]) and fibromyalgia [20]. By reducinganxiety pain improving sleep, hypnosis contributes significantly to the well-being of patients with these conditions. It is also used to alleviate the side effects of cancer treatments, particularly nausea and vomiting caused by chemotherapy and radiation therapy [21].
The benefits of hypnosis in medicine are undeniable. By combining this technique with other tools, such as virtual reality, we can explore new avenues for improving the management of pain anxiety. The immersive environments created by virtual reality enhance the effectiveness of hypnotic suggestions, thereby offering patients a more engaging and comprehensive therapeutic experience. To learn more about our services, visit this page.
The key takeaway
- Hypnosis is an altered state of consciousness characterized by focused attention and increased suggestibility.
- Medical hypnosis differs from hypnotherapy in that it takes place within a medical setting and follows standardized protocols.
- Hypnosis offers a non-medication-based approach to managing pain andanxiety and to relieve symptoms associated with chronic illnesses or cancer.
Further Reading
SFAR Statement on Hypnosedation:
The Different Schools of Hypnosis:
- https://www.hypnose.fr/hypnose/courants-hypnose-therapeutique/,
- https://books.google.fr/books?hl=en&lr=&id=en34AgAAQBAJ&oi=fnd&pg=PR3&dq=diff%C3%A9rents+types+d%27hypnose+m%C3%A9dicale&ots=Jzu4MHU-YJ&sig=flCz-A67neA0wJlduMMNtbuQFiI&redir_esc=y#v=onepage&q=diff%C3%A9rents%20types%20d'hypnose%20m%C3%A9dicale&f=false
Netflix Documentary:
Cover photo credit: My Voice Will Be With You
References
[1] G. R. Elkins, A. F. Barabasz, J. R. Council, and D. Spiegel, “Advancing Research and Practice: The Revised APA Division 30 Definition of Hypnosis,” Int. J. Clin. Exp. Hypn., vol. 63,no. 1, pp. 1–9, Jan. 2015, doi: 10.1080/00207144.2014.961870.
[2] A. Bioy, “Hypnosis and Hypnotherapy,” EMC - Psychiatr., vol. 1,no. 1, pp. 1–13, Jan. 2004, doi: 10.1016/S0246-1072(02)00083-4.
[3] G. De Benedittis, “Neural mechanisms of hypnosis and meditation,” J. Physiol.-Paris, vol. 109,no. 4–6, pp. 152–164, Dec. 2015, doi: 10.1016/j.jphysparis.2015.11.001.
[4] A. Vanhaudenhuyse et al., “Pain and non-pain processing during hypnosis: A thulium-YAG event-related fMRI study,” NeuroImage, vol. 47,no. 3, pp. 1047–1054, Sept. 2009, doi: 10.1016/j.neuroimage.2009.05.031.
[5] V. De Pascalis, “Brain Functional Correlates of Resting Hypnosis and Hypnotizability: A Review,” Brain Sci., vol. 14,no. 2, p. 115, Jan. 2024, doi: 10.3390/brainsci14020115.
[6] D. J. Acunzo, D. A. Oakley, and D. B. Terhune, “The neurochemistry of hypnotic suggestion,” Am. J. Clin. Hypn., vol. 63,no. 4, pp. 355–371, Apr. 2021, doi: 10.1080/00029157.2020.1865869.
[7] C. Kendrick et al., “Hypnosis for Acute Procedural Pain: A Critical Review,” Int. J. Clin. Exp. Hypn., vol. 64,no. 1, pp. 75–115, Jan. 2016, doi: 10.1080/00207144.2015.1099405.
[8] P. Langlois et al., “Hypnosis to manage musculoskeletal and neuropathic chronic pain: A systematic review and meta-analysis,” Neurosci. Biobehav. Rev., vol. 135, p. 104591, Apr. 2022, doi: 10.1016/j.neubiorev.2022.104591.
[9] J. Zeng, L. Wang, Q. Cai, J. Wu, and C. Zhou, “Effect of hypnosis before general anesthesia on postoperative outcomes in patients undergoing minor surgery for breast cancer: a systematic review and meta-analysis,” Gland Surg., vol. 11,no. 3, pp. 588–598, March 2022, doi: 10.21037/gs-22-114.
[10] K. Madden, P. Middleton, A. M. Cyna, M. Matthewson, and L. Jones, “Hypnosis for pain management during labor and childbirth,” Cochrane Database Syst. Rev., vol. 2016,no. 5, May 2016, doi: 10.1002/14651858.CD009356.pub3.
[11] M. Holler, S. Koranyi, B. Strauss, and J. Rosendahl, “Efficacy of Hypnosis in Adults Undergoing Surgical Procedures: A meta-analytic update,” Clin. Psychol. Rev., vol. 85, p. 102001, Apr. 2021, doi: 10.1016/j.cpr.2021.102001.
[12] I. Kirsch and S. J. Lynn, “The altered state of hypnosis: Changes in the theoretical landscape,” Am. Psychol., vol. 50,no. 10, pp. 846–858, Oct. 1995, doi: 10.1037/0003-066X.50.10.846.
[13] T. Thompson et al., “The effectiveness of hypnosis for pain relief: A systematic review and meta-analysis of 85 controlled experimental trials,” Neurosci. Biobehav. Rev., vol. 99, pp. 298–310, Apr. 2019, doi: 10.1016/j.neubiorev.2019.02.013.
[14] F. Bobin, C. Garreau, and J. R. Lechien, “Safety and Feasibility of Hypnosis-Induced Sleep Endoscopy in Patients with Obstructive Sleep Apnea,” Ear. Nose. Throat J., p. 014556132311700, Apr. 2023, doi: 10.1177/01455613231170094.
[15] F. Hızlı et al., “The Effects of Hypnotherapy During Transrectal Ultrasound-Guided Prostate Needle Biopsy on Pain and Anxiety,” Int. Urol. Nephrol., vol. 47,no. 11, pp. 1773–1777, Nov. 2015, doi: 10.1007/s11255-015-1111-0.
[16] G. Elkins, J. White, P. Patel, J. Marcus, M. M. Perfect, and G. H. Montgomery, “Hypnosis to Manage Anxiety and Pain Associated with Colonoscopy for Colorectal Cancer Screening: Case Studies and Possible Benefits,” Int. J. Clin. Exp. Hypn., vol. 54,no. 4, pp. 416–431, Dec. 2006, doi: 10.1080/00207140600856780.
[17] K. E. Valentine, L. S. Milling, L. J. Clark, and C. L. Moriarty, “The Efficacy of Hypnosis as a Treatment for Anxiety: A Meta-Analysis,” Int. J. Clin. Exp. Hypn., vol. 67,no. 3, pp. 336–363, July 2019, doi: 10.1080/00207144.2019.1613863.
[18] R. Schaefert, P. Klose, G. Moser, and W. Häuser, “Efficacy, Tolerability, and Safety of Hypnosis in Adult Irritable Bowel Syndrome: Systematic Review and Meta-Analysis,” Psychosom. Med., vol. 76,no. 5, pp. 389–398, June 2014, doi: 10.1097/PSY.0000000000000039.
[19] J. Bissonnette, E. Dumont, A.-M. Pinard, M. Landry, P. Rainville, and D. Ogez, “Hypnosis and music interventions for anxiety, pain, sleep, and well-being in palliative care: systematic review and meta-analysis,” BMJ Support. Palliat. Care, vol. 13,no. e3, pp. e503–e514, Dec. 2023, doi: 10.1136/bmjspcare-2022-003551.
[20] G. Elkins, “Efficacy of Hypnosis Interventions: Fibromyalgia, Sleep, Oncology, Test Anxiety, and Beliefs,” Int. J. Clin. Exp. Hypn., vol. 71,no. 4, pp. 273–275, Oct. 2023, doi: 10.1080/00207144.2023.2243785.
[21] J. Richardson, J. E. Smith, G. McCall, A. Richardson, K. Pilkington, and I. Kirsch, “Hypnosis for nausea and vomiting in cancer chemotherapy: a systematic review of the research evidence,” Eur. J. Cancer Care (Engl.), vol. 16,no. 5, pp. 402–412, Sept. 2007, doi: 10.1111/j.1365-2354.2006.00736.x.
Want to test Lumeen for 30 days with no commitment ?